Response to induction therapy is variable and many patients do not achieve fr a full response, even at 12 months1

50% of patients continue to use glucocorticoids 12 months after starting induction therapy1
12

Patient support organisations

ANCA involvement
Loss of immune tolerance to ANCA antigens and development of ANCA by plasma
cells 1
ANCA are most commonly directed against the neutrophil lysosomal enzymes PR3
and MPO in GPA and MPA, respectively 1–5 fr
ANCA involvement
Loss of immune tolerance to ANCA antigens and development of ANCA by plasma
cells 1 fr

Referral
consectetur adipisicing elit. Nesciunt consequuntur obcaecati provident illo
Diagnosis
sit amet consectetur adipisicing elit. Reprehenderit, nam. fr
AEs remain an issue for new and relapsing patients1,2 fr
Over the first 12 months of treatment in patients with GPA (Granulomatosis with Polyangiitis, previously called Wegener’s) or MPA (Microscopic Polyangiitis), AEs are common.1,2 At this time, glucocorticoid dose is typically highest, as current treatment guidelines recommend the use of GCs for remission induction.1–3 The majority of patients continue to use glucocorticoids 12 months after starting remission induction1,2 fr
New-patients (n=929)1




Relapsing-patients (n=268)1




Introduction to AAV! fr
AAV is a rare, severe small vessel vasculitis that affects multiple organs and has a high acute mortality risk1 fr
Read more fr
Introduction to AAV2
AAV is a rare, severe small vessel vasculitis that affects multiple organs and has a high acute mortality risk1
Read more
Introduction to AAV3
AAV is a rare, severe small vessel vasculitis that affects multiple organs and has a high acute mortality risk1
Read moreLatest clinical data in AAV fr
RAVEc fr
Rituximab (RTX) was found to be as effective as cyclophosphamide (CYC) for the induction and maintenance of remission, but remission rates remain variable fr
2010
RITAZAREM
Preliminary results show that a reduced glucocorticoid (GC) dose can be effective for reinducing remission in AAV. RTX was superior to azathioprine (AZA) at maintaining remission
2014
PEXIVAS
Reducing the GC dose in severe AAV patients did not significantly impact the primary outcome of death or end-stage renal disease, but did reduce the rate of infection (HR=0.69)
2018
ADVOCATE
Avacopan-based regimen is
non-inferior at achieving remission at Week 26 and superior at sustaining remission at Week 52 compared to a GC-based regimen1
2018
MAINRITSAN 1
RTX is more effective than AZA for maintenance of remission, but GC use and relapse remain common
2019
MAINRITSAN 2
Tailored and fixed-schedule RTX regimens are equally as effective at maintaining remission, but relapses still occur
2020
MAINRITSAN 3
RTX is more effective than AZA for maintenance of remission, but GC use and relapse remain common
2020
GPA and MPA patients accumulate organ damage from a combination of vasculitis activity and glucocorticoid-related AEs1–3 fr
Long-term and repeated high-dose glucocorticoid use is associated with an increased risk of new onset/worsening of diabetes mellitus, hypertension, osteoporosis, avascular necrosis of bone, malignancy, cataracts and other debilitating side effects.1,2*† In a study following newly diagnosed GPA and MPA patients for up to 7 years, the frequency of damage, including potentially treatment-related damage, rose over time (p<0.01). Patients initially experience early increased damage following diagnosis (n=270), with 81.5% of patients experiencing ≥1 item in the VDI at 6 months compared to 24.4% of patients at baseline, with renal (proteinuria and GFR <50 mL/minute) and cardiovascular (hypertension) damage the most frequent. Severe damage, a VDI score ≥5, increases over time and at long-term follow-up 33.7% of patients had severe damage. Hypertension was the most commonly reported item at long-term follow-up, demonstrating an accumulation of cardiovascular damage over time. At baseline, 4.8% of patients had hypertension. Within 6 months, this rose to 17.0% and at long-term follow-up 41.5% of patients had hypertension (p < 0.01 ).2†
High levels of long-term vasculitis damage were independently associated with increased cumulative glucocorticoid use (p=0.016).3†
This serious morbidity is accompanied by a significantly increased long-term mortality risk, with a hazard ratio of 2.41 (95% CI: 1.74–3.34) in GPA patients compared with age- and sex-matched controls.2–4†‡fr
At a mean of 7 years post diagnosis in patients with GPA or MPA…2†

Referral, diagnosis & follow-up
AAV patients often experience a complex pathway of patient referral and diagnosis1*
EULAR recommendations state that patients should have access to education focusing on the impact of AAV and its prognosis, key warning symptoms and treatment (including treatment-related complications). AAV requires multidisciplinary management by centres with, or with ready access to, specific vasculitis expertise.2

Many patients have renal disease at presentation, but general non-specific referral symptoms predominate1
Renal disease: 64%
Fatigue: 58%
Fever: 54%
Weight loss:53%
Joint pain: 47%
16% of patients have had their referral symptoms for over 3 months before receiving an AAV diagnosis1
Comorbidities at diagnosis are common (65% of patients)1
Hypertension:45%
Type 2 diabetes:16%
COPD/asthma:15%
Coronary arterial disease:10%
Arthritis:9%
Osteoporosis:7%
BMI >35:6%
Cardiac failure:6%
Discover the key clinical data in AAV
Our current understanding of patient outcomes in ANCA-associated vasculitis (AAV) is rapidly evolving as more studies are being conducted.
to read the key clinical research papers to find out more about treatment outcomes in AAV.
click here
Treatment-related AEs are the leading cause of acute mortality1
In the first year after a GPA or MPA diagnosis, 56 of 524 patients died. A total of 59% of these deaths were as a result of treatment-related AEs.1*
A systematic literature review of glucocorticoid-related AEs in AAV clinical studies published between 1 January 2007 and 30 January 2018 identified mortality (33%) as the glucocorticoid-related serious AE with the highest frequency observed during early induction treatment. Other common glucocorticoid-related serious AEs experienced by patients include infections (20%), musculoskeletal (17%) and renal disorders (15%).†

The development of AAV is a complex and multifactorial autoimmune process2,3
The initial causes of AAV are currently unclear.3 Predisposing factors such as microbial infection, genetic influence, environmental agents and specific drugs are all fundamental to the development of AAV.2,3
Exposure to silica, pesticides, fumes, construction materials, hydrocarbon (cleaning agents, paint, diesel), drugs (propylthiouracil, hydralazine, D-penicillamine, cefotaxime, minocycline, anti-TNF agents, phenytoin) and certain psychoactive agents may all cause AAV.2,3
INTRODUCING AAV WORLD!
Balancing different clinical priorities is a major challenge in the management of ANCA-associated vasculitis: keep inflammation under control, achieve and sustain remission, prevent long-term organ damage, all while navigating treatment options that in their own way may place a heavy burden on patients.1–3
We think it’s important to have a chance to learn, while also relaxing! AAV World is a brand-new educational game that sheds light on the clinical priorities in AAV in a fun and interactive way, through a mix of skills challenges, brainteasers, riddles and quizzes.
Your objective: protect AAV World from damage
Start by viewing the AAV World landscape and decide which of the four zones is your most urgent priority:
- Vasculitis Volcano represents vasculitis activity
- Burden Forest represents the burden that comes with the disease and treatment
- Patient Metropolis represents the patients experience and their quality of life
- Kidney Island represents organ damage
Complete interactive challenges, brainteasers, riddles and quizzes. Each time you win, you’ll be improving the health of AAV World.
you up to the challenge? Protect AAV World today!
Play Now References & footnotes
Join the Rare Disease Investigation Team to help think what may be causing an unusual, but highly dangerous situation.
You’ll need to examine the evidence – reading case files on the impact of AAV, impact of treatment and delay to diagnosis, as well as watching highly classified CCTV footage.
Can you identify the prime suspects before the time runs out?

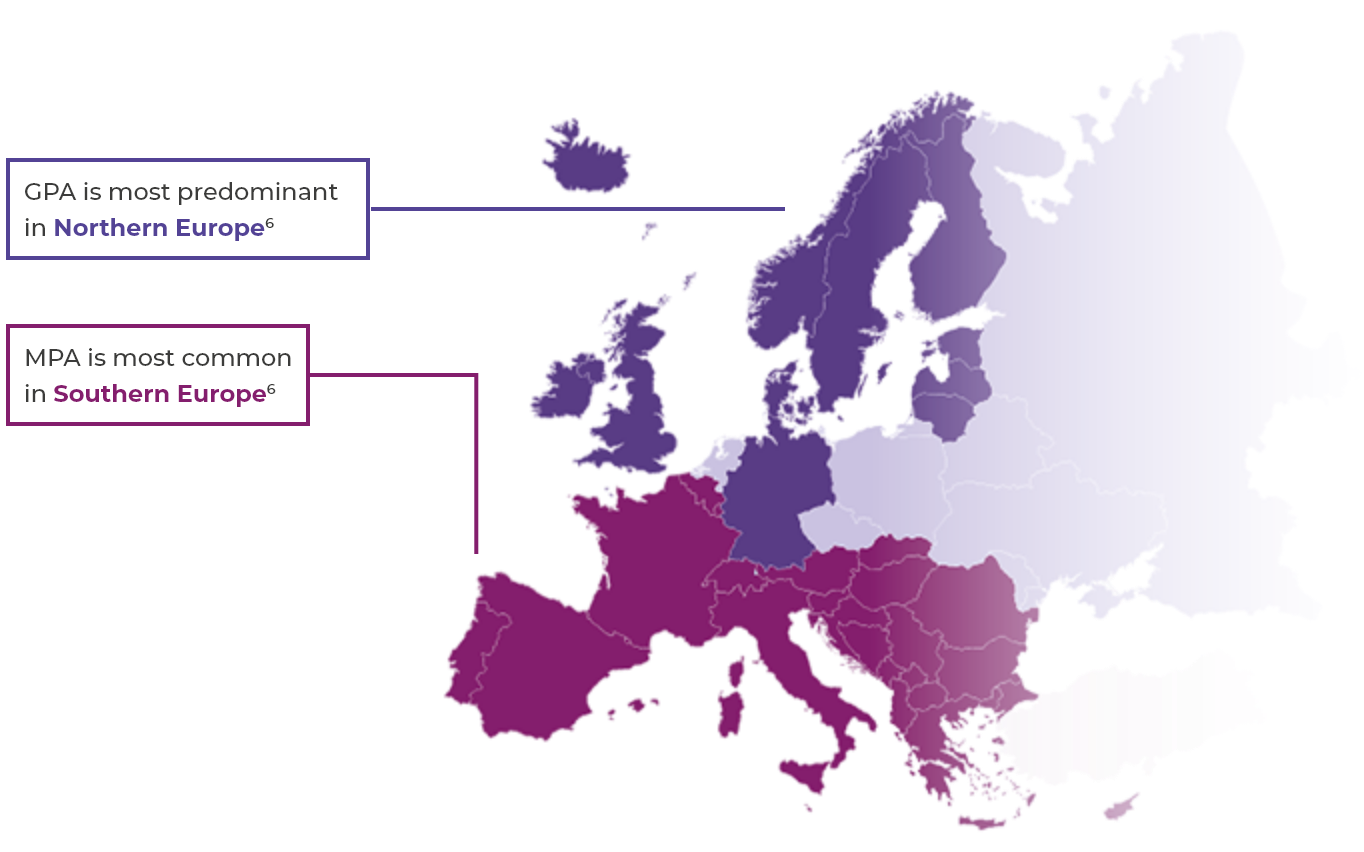
Incidence & prevalence
Types of AAV
The two most common subtypes of AAV are granulomatosis with polyangiitis (GPA, previously called Wegener’s) and microscopic polyangiitis (MPA). The other subtype is eosinophilic granulomatosis with polyangiitis (EGPA, previously called Churg-Strauss syndrome).2,3 This website will focus mainly on GPA and MPA.
AAV is a rare disease2
- Global prevalence: 30–218 per million4
- European incidence: 13–20 per million per year2,4
AAV occurrence
- AAV can affect both younger and older people, but is rare in children and young people and incidence rises with age2,5
- AAV occurs slightly more frequently in men (annual incidence rate approximately 60%) than in women2,5